


 (Photo: Unsplash)
(Photo: Unsplash) The SA government has just passed National Health Insurance legislation and with a heavy heart, I have to admit, I’m against it. I’ll get to the reasons in a moment, but it’s worth reflecting on the arguments from the other side, because they are considerable.
The most important argument emanates from simple equity: life is unfair in so many ways, but in principle, everyone should have access to the healthcare they need on a more or less equal basis, and the costs should be borne in proportion to wealth. I think that is pretty obvious.
But there is much, much more to it than that. The biggest problem with healthcare from a free-market point of view is that this is an industry where there is a huge information asymmetry. The consequence is that the ability of ordinary people to decide what their best interests are is extremely difficult (but not impossible) to do. You can judge pretty easily the value of one car over another because a host of information is available to you: the engine capacity, the size, the make, the cost; you name it, the info is there.
But if your doctor suggests you should take Panado rather than aspirin, or neither, or both, your ability to judge whether she is right is a tricky question. Even questions about whether to take vaccines, which I think is pretty much an open and shut case, have engendered a huge debate recently, though the information to make an informed decision is more or less readily available.
US vs UK health systems
The result is that even for free market supporters like me, healthcare is a tricky area, and I’m prepared, reluctantly, to concede there may indeed be reasons that market distortions can filter into the system. The best example comes from a simple comparison between a predominantly state-controlled system, like the National Health Service in the UK, and a broadly private system like in the US.
See the table below: the US spends an absolutely huge 18.82% of its enormous GDP on healthcare, and the UK spends only around 12%. But the UK’s healthcare outcomes are more or less the same; you can see from the graph that life expectancy – one major healthcare outcome – is actually higher in the UK than in the US.
I have also tabulated the excess deaths over the Covid period, and as you can see, the UK outperformed the US, not by a huge margin but it is noticeable. It’s certainly evident if you consider that the UK is spending $5,350 a year per person on the population while the US spends roughly three times that. Germany spends even more and gets more or less the same results.
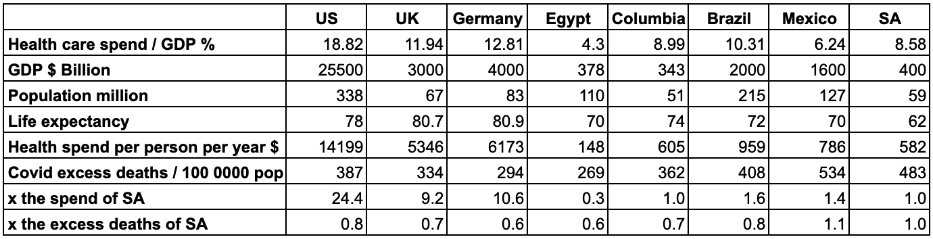
South Africa spends about 8.5% of GDP on health, and it’s hugely weighted toward the wealthy. The country spends R277-billion on healthcare in the private sector, used by 16% of the population, and R265-billion on healthcare in the public sector, used by 84%. Arguably, SA has the worst of both systems: a dysfunctional public healthcare system and a massively expensive private healthcare system. So, case closed? Not so fast.
One thing that intrigued me was the effect of the Covid pandemic. The pandemic was a huge challenge to healthcare systems around the world, and it’s interesting to measure the countries that came out of it best. The figures I’m using are excess deaths, because that captures not only Covid deaths but people who died from other problems since hospitals were so stretched by Covid. Excess deaths have the utility of being specific and easier to quantify than, say, certified Covid deaths.
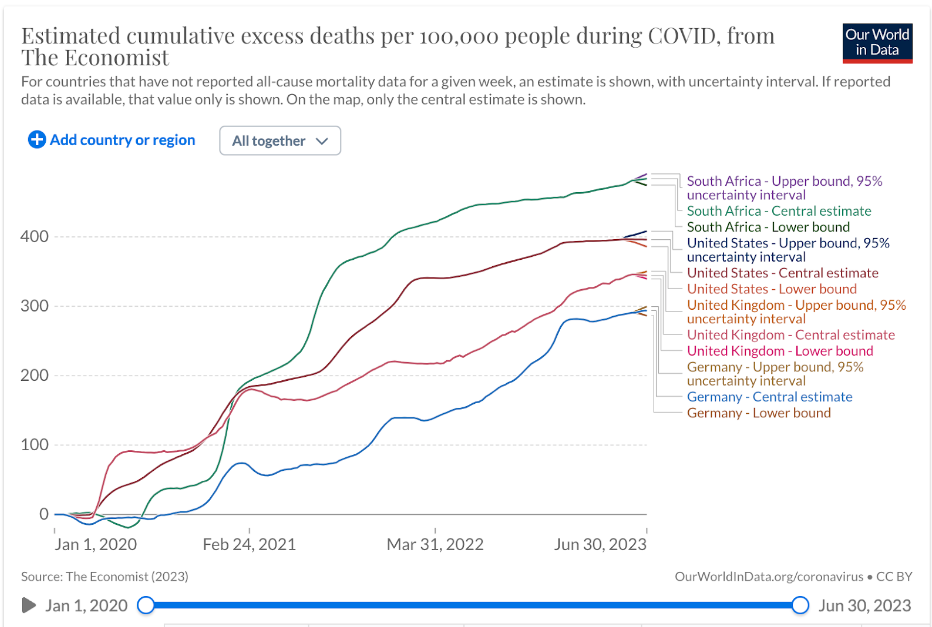
And you know, when you look at it, SA didn’t come out of the crisis badly. Maybe there is more to be said for SA’s partly public and partly private system than it seems. For example, SA outperformed the US on money spent versus excess deaths; indeed all countries did better than the US because the healthcare spend part of the equation is so inflated in the US.
But it’s still eye-popping how much better SA did than the developed world on the same measure: the UK, for example, spends nine times more per person than SA but suffered only 30% fewer deaths. The same, more or less, applied to Germany. But what about the developing world? SA’s performance compared to its peers is pretty much the same. SA spends roughly the same, per person, as Colombia, and the number of excess deaths per thousand was almost the same – even though Colombia has a “free at the point of use” system.
More money doesn’t mean better healthcare
The only real conclusion you can draw from all of this is that the correlation between healthcare outcomes, healthcare systems and money spent just doesn’t exist. The way to improve healthcare is not, it turns out, to throw money at it.
And that leads me to worry that if the SA government were to double the amount it spends on healthcare by absorbing the amount spent now by the private sector into the government sector, would poor people necessarily get a better service? This is the logic implicit in the NHI Act.
I just don’t think they will. That’s not how government services work, certainly not in SA. The way that the government works means state-owned enterprises (SOES) or government departments start functioning not as a service to the population as a whole but predominantly as a service to government and SOE employees.
The South African medical profession is hugely opposed to the NHI Bill, but you know, they shouldn’t be, because they are going to make out like bandits. Doctors in the UK’s public system earn quite a lot less, on average, than doctors in the US, but much, much more than doctors in SA’s private system. UK doctors earn about the same as French doctors, but quite a lot less than German doctors. Once again, there is little correlation between money and system.
This is not to say there isn’t a problem with overcharging on the private sector side of the equation; I’m shocked that I have to fork out about 10% of my take-home pay for my very basic private healthcare insurance. But as much as I complain, it is extraordinary how much innovation and forward thinking there is in SA’s private healthcare system, and as a society, we are so much better off for it.
Dependence on US spending
There is also an argument linked to how much the US is paying for its largely private system: what if this is not a mistake, but a virtue. What if public systems around the world are essentially being subsidised by the US?
For example, Pfizer makes about half its profits in the US, and only about a quarter in Europe, despite the population of Europe being three times that of the US. If the US had a purely public system, wouldn’t the Europeans end up paying more for pharmaceuticals, assuming the same level of profitability and the same health delivery? Well, you could say, Pfizer would just have to settle for lower profits. But the problem is that pharmaceutical companies actually don’t make much larger profits than most other companies, on average. They certainly make much less, as a proportion of turnover, than tech companies.
The uncomfortable fact is that the entire global healthcare industry depends on the US spending freely on healthcare – SA included, and this is another thing the Covid crisis demonstrated. Vaccines developed with largely US scientific technology, and certainly distributed with US corporate heft, were massively more effective than competing systems, including massively well-funded and highly motivated public systems. Public systems have huge amounts to learn from private companies, and without them we would all be worse off.
This is an enormously hard question and is unresolved internationally, and it pains me to vote against a fairer system. If the government were just better and more sensible in its administration of the existing public healthcare (or anything it manages, for that matter) it would make the decision so much easier. Ultimately, I think there has to be a way to structure the industry that doesn’t destroy the private sector in favour of the public sector – or the other way around. DM