


The Portfolio Committee on Health (PCH) heard oral presentations on the National Health Insurance Bill (the bill) from 116 individuals, organisations and institutions from 18 May 2021 to 23 February 2022. What the PCH will take from these diverse public inputs as it presents a final bill to the National Assembly for voting on, remains to be seen.
However, to clarify insights and advice, and to inform their deliberations on the NHI, the PCH now has information from all presentations, collated by the Parliamentary Monitoring Group and systematically examined by researchers from the South African Medical and Research Council, the Clinton Health Access Initiative, the University of the Western Cape and the University of Cape Town.
This article examines the views presented by different organisations on the financing proposals in the bill.
Current and NHI-proposed funding models
Globally, a range of healthcare funding models exist, from those relying mainly on private funding (individuals pay out of pocket or buy private insurance), to those relying on public funding (state pays using tax contributions).
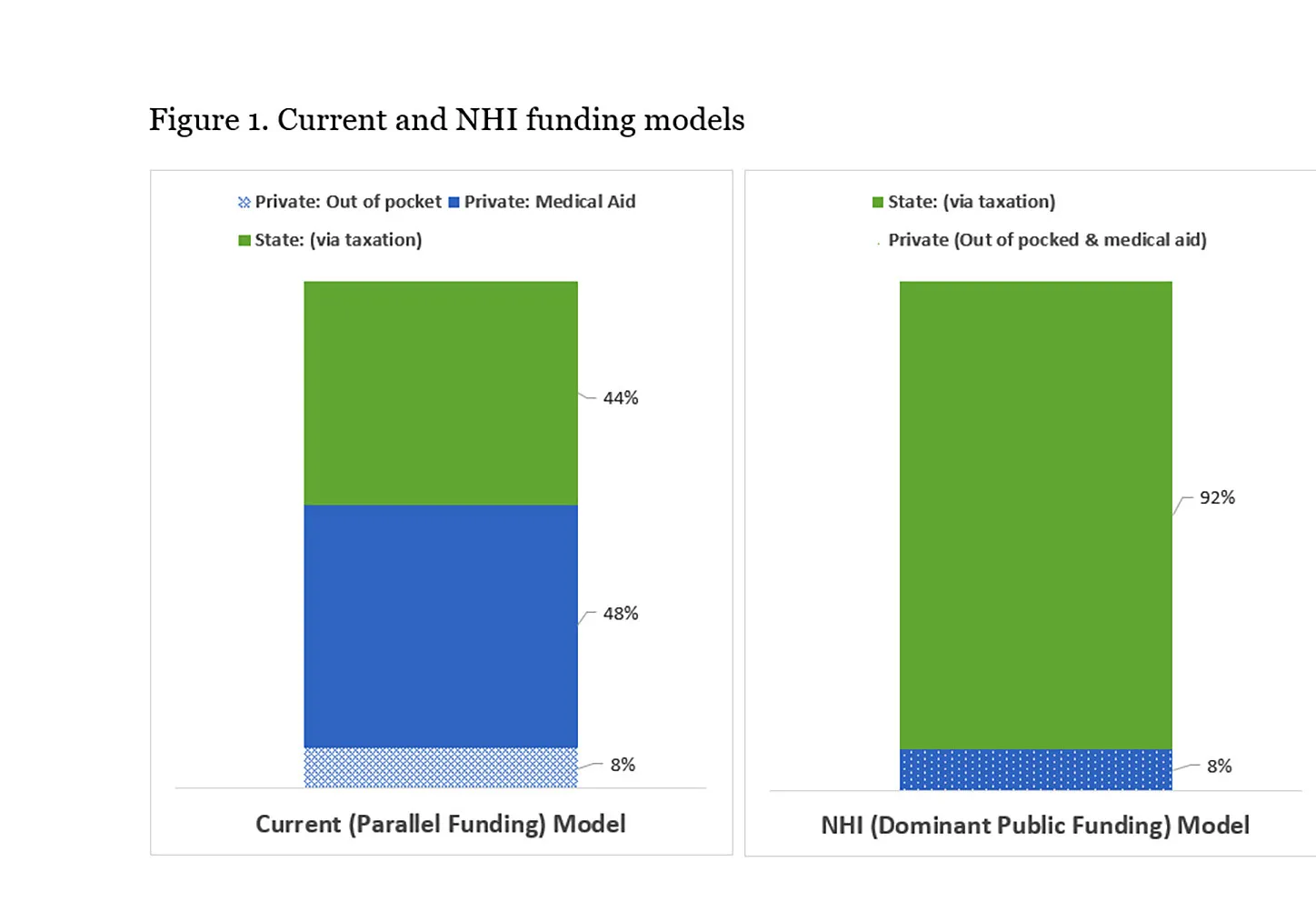
South Africa currently operates a “parallel” funding model with about 44% of healthcare expenditure funded by tax-based state funding, 48% by individuals via private medical aids and 8% by “out of pocket” payments. The bill entails moving to a “dominant public funding” model by moving “private funding” to “public funding” (Figure 1). Public funding would increase mainly via an increase in taxes, while private funding would decrease as the NHI is expected to cover all or most healthcare needs and expenditures, and private medical aids would only be allowed to cover benefits excluded by the NHI.
Support for the NHI funding model
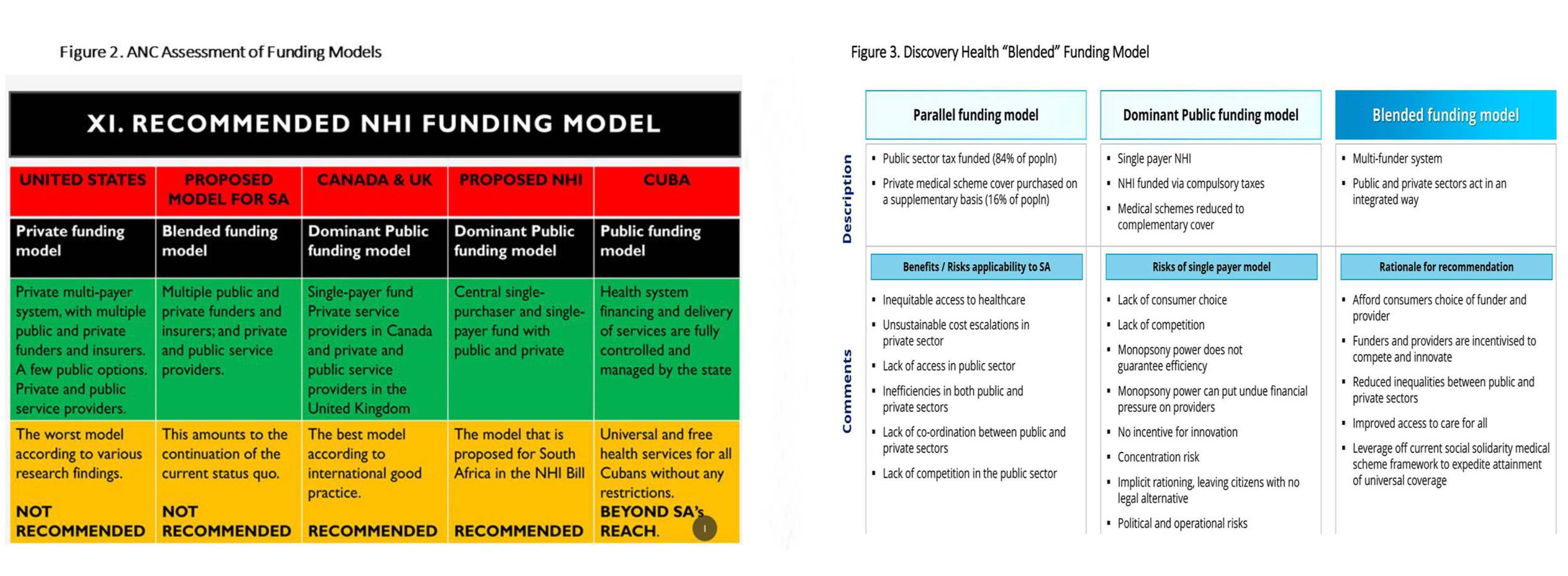
Those backing the bill see the NHI funding model as the mechanism to address inequities and inefficiencies in South African healthcare (Figure 2). The ANC claims the “National Health Insurance is a health financing system designed to pool funds and actively purchase services with these funds to provide universal access to quality, affordable personal health services for all South Africans based on their health needs, irrespective of their socioeconomic status”. Underlying its support is the view that the shift to a “public-dominant” funding model will translate into greater public control of health financing, a better integrated healthcare system, greater cross-subsidation, concentrated purchasing power and enhanced purchasing efficiency.
The question of how public funding will be increased to about 8% of GDP is an area of contention. Section 49 of the bill states that the NHI will be funded from the reallocation of medical scheme tax credits, general tax revenue, payroll tax and a surcharge on personal income tax.
Among supporters of the bill there is widespread support for the reallocation of medical scheme tax credit funding, with Nehawu arguing that “as part of funding for the NHI, government should completely end tax rebates to medical scheme holders… government should redirect tax rebates towards the NHI fund”.
However, on the issue of increased taxation, views were a bit more mixed. The ANC endorsed the sources of funding stated in the bill and called for “the money currently available in the public and private sector for personal health services (to be) supplemented by money from the fiscus”, arguing that this debunks the myth of extra taxation.
Cosatu, on the other hand, called for extra taxation, arguing that “the tax net will need to be expanded and made more progressive and new taxes targeted at the wealthy”. It further argued for a mandatory enrolment and mandatory prepayment arrangement, a payroll tax on employers, a progressive tax on wages, financial assets and investments of the wealthy, tax on inheritance and estate duties, and taxes on luxury imports, currency transactions and financial transactions.
Five major concerns with the NHI funding model
Those opposing the NHI funding model were concerned (1) that the bill did not provide sufficient detail on how the funds will be raised, (2) that the increased taxation was unaffordable or unsustainable, (3) that the bill was not clear on how funding will flow to providers, and (4) did not believe that the public-dominant funding model would work in South Africa and/or (5) there were better funding models.
Lack of detail was a recurring concern.
/file/dailymaverick/wp-content/uploads/2022/03/MC-NHIOped-1_3.jpg "There was broad support for the rhetorical aim of the bill to bring universal healthcare to all, but many doubted whether the strategies set out in the bill could deliver this. (Photo: Gallo Images / Foto24 / Lulama Zenzile)")
The Alliance of South African Independent Practitioners Associations said that “not enough detail is given as to the financial viability of the NHI Fund”. Bonitas pointed out that “apart from Section 49(2)(a), there is no clarity in terms of how the NHI will be funded”. The National Planning Commission said it “reserves its full comments on the funding aspects until such time as further details have been made available for comment”.
Increasing taxes was expressed as either unaffordable or unsustainable. The University of the Witwatersrand (Wits) said “the fiscal requirements for the substitution of medical schemes contributions with general tax increases is plainly unachievable”.
Discovery Health pointed out that the increased taxation (4.1% of GDP) required to shift the R212-billion currently spent by nine million South Africans on medical aid cover from “private” to “public” is unlikely to be feasible. While the removal of medical tax credits would release funding of R26-billion to R29-billion, the remainder of the shortfall that would need to be funded through increased taxation would still be very substantial.
The DA similarly felt ordinary South Africans have been squeezed dry by government taxes and cannot be subjected to yet another tax. The bill was fiscally irresponsible, given the projected R380-billion deficit in the Main Budget Framework, so it was questionable whether the state could afford the NHI. They noted that “many respectable economists have warned that the NHI will hurt our already ailing economy and increase our debt”.
Among those opposed to a “public-dominant” funding model, Discovery Health argued that the single-payer model would reduce consumer choice, competition and efficiency. It would also put undue financial pressure on providers, concentrate risk, lead to implicit rationing and carry political and operational risks.
The DA argues that the “bill removes the autonomy of South Africans to choose their own healthcare. It mandates the national Department of Health as the sole provider of healthcare in the country while all private healthcare providers will be contracted by the state. This means that there is absolutely no choice for people on which services to purchase, nor will there ever be competition to drive up the quality of healthcare”. They further argue that the “pooling of funds is essentially throwing money at a problem without fixing the challenges. It is unclear how the fund will be protected from theft, mismanagement and corruption. A pooled fund will not equate to improving the efficiency of the healthcare system.”
The DA went on to recommend that “The Department of Health should focus on fixing governance and management structures to increase efficiency and accountability of the public healthcare system before considering an NHI”.
The National Planning Commission, in raising concerns about the institutional arrangements and powers of the minister, noted that “the bill appears to be drafted on the assumption of a perfectly efficient, ethical, and capable state, and tends to ignore the reality of inadequate public healthcare services”.
The Board of Health Care Funders identified a lack of clarity on how funds will flow to providers as an area of concern. They argued that there was no provision for the payment of funds to provincial health departments and municipalities for services they render, and no distinction made between basic services they were constitutionally obliged to fund from their equitable share of national revenue, and NHI-funded health services. Currently, provincial health departments are responsible for health service delivery, in terms of Schedule 4 (health services) and Schedule 5 (ambulance services) of the Constitution. While the Bill makes provision in the schedule for laws to be amended, the constitution cannot be amended in this manner.
Proposals on alternatives
The purpose of the hearings was also for respondents to table suggestions.
Discovery Health was one of the few respondents that considered and tabled an alternative “blended” funding model with a multifunder system in which the public and private sectors act in an integrated manner, as well as the rationale for it. This is summarised in Figure 3.
Portfolio committee response
There was broad support for the rhetorical aim of the bill to bring universal healthcare to all, but many doubted whether the strategies set out in the bill could deliver this.
The choice of a financing model capable of supporting the proposed NHI reforms is critical to the success of the whole NHI initiative, but there were strongly divergent views on the viability of shifting from the current funding model to the proposed public-dominant funding model, for which little tangible evidence or detail had been made available.
The PCH will need to consider whether this deficiency of detail limits its endorsement of the bill in its current form, or prompts it to address this critical information deficit.
The NHI Bill is one of the largest reforms proposed since 1994 and the approach taken by the PCH on its financing in particular will have a profound impact not only on the future health system but also on the broader trajectory of social, societal and economic wellbeing in South Africa. DM/MC
Geetesh Solanki is Specialist Scientist at the Health Systems Research Unit, SA Medical Research Council (SAMRC); an Honorary Research Associate in the Health Economics Unit, University of Cape Town and Principal Consultant at NMG Consultants and Actuaries; Neil Myburgh in a Professor in the Department of Community Dentistry, Faculty of Dentistry and WHO Collaborating Centre for Oral Health, UWC. Stephanie Wild is a postgraduate student enrolled for a MPhil in Public Law at the University of Cape Town; Judith Cornell is a former Director of Institutional Development and Planning (retired) at the Nelson Mandela School of Public Governance, University of Cape Town; Vishal Brijlal is a Senior Director at the Clinton Health Access Initiative.
The opinions expressed are those of the authors and do not necessarily reflect the views of their institutions.