



 A Chinese passenger that just arrived on the last bullet train from Wuhan to Beijing is checked for a fever by a health worker at a Beijing railway station on January 23, 2020 in Beijing, China. (Photo: Kevin Frayer/Getty Images)
A Chinese passenger that just arrived on the last bullet train from Wuhan to Beijing is checked for a fever by a health worker at a Beijing railway station on January 23, 2020 in Beijing, China. (Photo: Kevin Frayer/Getty Images) The recent emergence of the new coronavirus (Covid-19) in China comes as no surprise to infectious disease specialists, who have warned of the inevitability of this occurrence for decades. Many viral infections, such as influenza, Ebola, rabies and SARS are transmitted to humans from animals, and our increasing exposure to animals over time adds to the risk of more animal-to-human transmissions.
The current Covid-19 outbreak in China is a serious concern for the entire world, despite the epidemic being almost exclusively in China, with relatively limited spread elsewhere.
The WHO is an inherently conservative body that does not declare outbreaks a “Public Health Emergency of International Concern (PHEIC),” without reason. Its expert committees deliberated and declared the Covid-19 outbreak to be a PHEIC at the end of January.
Today’s figures show that there are 75,725 identified cases in the world, of which 98.5% are in mainland China. Of the 1,149 identified cases outside China, about half were identified on a single cruise liner, the Diamond Princess. Only one case has been confirmed in Africa, that being in Cairo, Egypt, and about 500 other confirmed cases are scattered across the globe. There have been 2150 deaths recorded, almost all in China. The map below gives a visual description of the spread, showing the very limited number of cases outside of China.

That should not lull anyone into the misconception that this is not a major pandemic that is possibly in-development. There are two key elements that determine whether this has the potential to become a global pandemic, both of which have been fulfilled. First, the infectious agent needs to cross from another species to humans (which is a rare event); and second, it needs to spread reasonably easily between people.
Every indication since it was first identified in December 2019 points to the fact that it made its initial “jump” from an unproven animal species to humans in a wet market in Wuhan, Hubei Province, whereafter it has spread from person-to-person.
So-called “wet markets” in China are notorious for having thousands of live, wild animals from across the globe crammed in cages in very close proximity to the market sellers and customers, increasing the chances of a leap between species.
The massive international trade volumes in wild animals to China (and elsewhere) means that there is now greater chance of inter-species transfer of viruses, as people are getting more frequent contact with animals that were never handled and/or eaten before.
We are scrambling to learn more about the Covid-19 clinical picture. Data published this week in the Chinese Journal of Epidemiology reported on more than 72,000 cases in China, of which about half were laboratory confirmed cases. This work assists tremendously. There is no doubt that this is a disease of importance clinically.
However, one piece of information that remains elusive is what proportions of those infected have mild, severe or life-threatening illnesses. It is entirely possible that many of those infected with Covid-19 – like other human coronavirus infections – may have such a mild disease (or no symptoms at all) that they are not even noticed. If that is the case, then the percentage of those infected who develop serious disease will drop, as we learn more.
Based on the current data published, it appears clear that more than 80% of the cases in China have been mild, and only less than 5% have severe or life-threatening severity of Covid-19 disease. A yet-to-be-developed serological test that looks for antibodies to the virus in the blood of the general population is needed to determine this percentage of the population with asymptomatic disease with accuracy.
There are also striking differences in overall mortality within China, and early concerns of a very high mortality rate similar to SARS (8%) or MERS (>34%) – both also coronaviruses – have fortunately not been correct.
There is a mortality rate in Hubei Province of approximately 2.9%, while other Chinese provinces appear to have a mortality of 0.4%. The mortality figures also suggest that, like influenza, there are specific groups that are far more likely to have severe symptoms or die. Men, those with diabetes, hypertension or chronic respiratory diseases are more at risk of severe disease. There is a striking association between age and severity, with not a single death recorded in children under nine years of age. The Chinese Journal of Epidemiology reported the following mortality by age:
| Age | Mortality |
| 40-49 | 0.4% |
| 50-59 | 1.3% |
| 60-69 | 3.6% |
| 70-79 | 8% |
| >80 | 14.8% |
The research also points to the risk for infection in medical staff. China has had 3,019 health workers infected, of whom five have died.
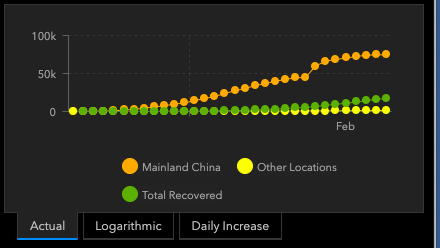
Where is this going? We have to be cautious at this stage, but the figure below (from the same source as the figure above) may suggest that the epidemic curve for China is “flattening out,” suggesting that the number of new cases is diminishing. That is good news, and may in part be due to the Chinese controls placed on movement between/within cities, or to a natural peaking of infections in those populations, or both.
Modelling suggests that the peak of new infections in China was in late January. The big jump demonstrated below on February 12-13 was due to a change in the “case definition” as to who was counted as infected, and thus does not reflect a true increase in the numbers.
The rest of the world is correct to be very worried that a spread to more areas will result in a global pandemic. Of particular concern is the spread of Covid-19 to developing countries with poor infrastructures, where many cases may go undetected on account of inadequate health structures, staffing numbers, laboratories and systems.
The introduction of Covid-19 to resource-poor environments where many people are poorly nourished and/or sick with other diseases such as hypertension, diabetes, TB, lung disease, and/or HIV may allow for a more rapid spread as well as more severe disease. These are issues that the continent will have to face with time.
There have been no confirmed cases of Covid-19 infection in South Africa. However, as with other coronaviruses and influenza viruses that have infected humans for millennia, these are more common in winter. Thus, when the temperatures drop as we approach winter, there is a higher likelihood of any introductions of this virus spreading in the region.
Where is SA in all this? SA has a public health system that has many challenges, but has a countrywide network of health facilities with universal access. Laboratory diagnostic testing is performed by the National Health Laboratory Service (NHLS), that services the entire country. The NHLS does this through its internal division, the National Institute for Communicable Diseases, that is tasked with conducting surveillance for Covid-19 as well as managing potential cases. Its highly qualified staff, its extensive sophisticated laboratory systems and an emergency operations centre, mean that it was one of the first to set up laboratory tests for Covid-19 on the continent as well as have a call centre to help identify any suspected cases.
Suspected cases and samples of nasal and throat swabs are handled according to a national protocol. Those who are confirmed as infected would be transitioned into isolation units which already exist for diseases such as Congo-Crimean Haemorrhagic Virus infections. Family, work and social contacts of confirmed cases would be screened and/or self-quarantined until they are shown to be negative. This is linked to a major effort at all ports of entry to screen for travellers with high fever, and the government has a formal, inter-sectoral plan on how it responds appropriately to Covid-19.
It is the opinion of many experts that the Chinese authorities will be unable to maintain the current dramatic clampdown of personal movement, work activities and transportation that is in place in much of China. Those who have stayed away from work and been refused permission to travel will have to return to their normal workplaces and be allowed to travel nationally and internationally. That may see increases in infections both in China, and in places internationally where Chinese travel for tourism and work.
It seems inevitable that Africa will have Covid-19 infections, as more than one million Chinese nationals are living and working in Africa, some of whom regularly travel back to the Chinese mainland. We need to be prepared for that.
Even if Covid-19 infections are generally mild, it is not the same as a simple cold. There is a relatively low, but significant hospitalisation rate, and death. Thus, we have to be prepared as well as proportionate in the country’s responses.
Being proportionate is critical, as this is not the only respiratory illness we are faced with annually. As reported in the medical literature, SA has more than 128,000 influenza infections every year, resulting in 11,000 deaths in 2019, despite an influenza vaccine being available.
The WHO estimates that there are as many as 650,000 deaths worldwide linked to influenza virus infections each year. Thus, the response to Covid-19 should be rational, and use the existing infrastructure and systems available that are so critical for other similar epidemics such as influenza.
Every effort should be made to contain and limit Covid-19 infections in SA, as our circumstances are different to other parts of the world.
One factor that we do not yet know is what effect the very poor living conditions and the role of other infections such as HIV, TB and malaria in much of Africa will do to influence the spread and seriousness of future Covid-19 epidemics in Africa.
While Chinese epidemiologists are reporting the mortality above, these may be very different in communities where there is a high prevalence of diseases affecting the immune system, in addition to the risk factors of age, diabetes, hypertension, etc.
We know that people with HIV have increased disease severity and mortality from influenza. While SA has a massive HIV treatment programme with about five million people on antiretrovirals, there are another two million who do not access these, and their altered immune systems may cause severe Covid-19 disease and increased death rate.
As China’s HIV epidemic is so different in this regard, we do not know the answer to this question of coinfection severity yet.
Africa is responding to this epidemic, with the Africa Centres for Disease Control and Prevention (Africa CDC) ramping up the continental capacity for laboratory testing and clinical surveillance. These efforts are critical.
Next month’s International Conference on Emerging Infectious Diseases hosted by the Africa CDC in Addis Ababa is perfectly timed for discussions on an appropriate continental response to Covid-19. Various high-level roundtable discussions on this issue will be very prominent at the meeting, and feedback on crucial interventions and surveillance to every African country is important.
And so, as the pilot informs us of her intent to start the descent into beautiful Cape Town, I feel more at ease that there is no need to wear a face mask on flights – yet. We may need that later, and I may scout around for a mask for future travel, if/when Covid-19 becomes a daily reality and disease of importance in the region. My fellow passengers’ desire to protect themselves is admirable. We all need to be vigilant. MC
Tim Tucker is a clinical virologist, and CEO of SEAD Consulting, a public health management consultancy. He is also an adjunct associate professor in the University of Cape Town School of Public Health and Family Medicine.
Comments
Scroll down to load comments...