



Since time immemorial, childbirth has been one of the most frightening yet beautiful moments in a woman’s life. At its core, childbirth is an incredible event that is, in every sense, what makes us human. Children born naturally, and without unnecessary medical intervention, are delivered into this world in the same way as so many billions who came before them. And for 99.99% of human history, natural birth was the only option.
But, for the longest of times it was also one of the most dangerous things a woman could do – history has lost count of all the women lost over the past centuries to childbirth-related ailments. Today, many think of C-sections as reducing this danger, but go back a century or two and you will find that C-sections were treated as an absolute last resort.
Historically, and even dating back to ancient Roman times, this procedure was performed to save the baby rather than the mother. In fact, it was only in 1580 that the first case of a mother surviving the surgery was actually recorded.
Yet, the dawn of the 21st century saw modern medicine advance beyond humanity’s wildest dreams. The C-section quickly became considered a low-risk procedure, afforded to almost any expectant mother, regardless of complications or lack thereof. A procedure that was designed to be used as a last resort, only when natural birth placed mother or baby at risk, might now be considered the preferred method of delivery, if I look at the statistics to which my company has access.
The question has become: Why go through the trauma of natural birth?
The World Health Organization (WHO) has found that C-sections now account for more than one in five (or 21%) of all childbirths across the globe. The WHO believes this number will continue to rise in the next decade to encompass 29% of all births by 2030. Right now, though, South Africa is worryingly ahead of this trend, to a point that is alarming.
Data from Medscheme shows that C-section deliveries more than doubled that of normal births between 2016 and 2020. With 3.9 million members, this provides an adequate sample of medically insured child-bearing South African women. While the WHO may be worried about 29% of global births becoming C-sections by 2030, our statistics show that C-sections account for 70% of all births on our medical schemes.
This makes the C-section rate among South African medical scheme members the highest rate in the world.
Our numbers also do not show any sustained impact of Covid-19 on births or the choice between natural/C-section. There was a marginal decrease in the number of C-sections admission in early 2021 during SA’s level 5 lockdown, but this was not maintained. Rather the reduction in admissions follows a gradual downward trend year on year for both C-sections and normal deliveries.
But what is causing such high instances of C-sections in South Africa? And, more importantly, what if anything should we do about it?
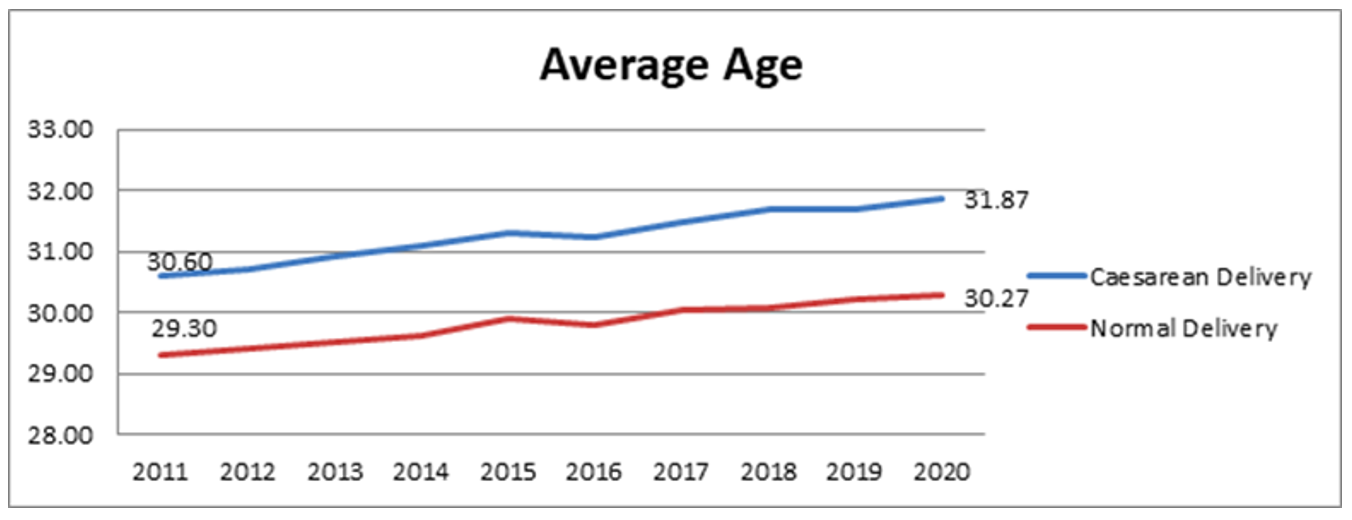
Again, I look to our data. Maternity events recorded between 2011 and 2020 show that women are progressively giving birth at older ages. The average age of a mother delivering a baby gradually increased by 1.3 years over a nine-year period.
Why this is, I can only speculate: much has been reported on the fact that women are becoming more career-driven, and want to focus on their professional life by being more competitive in the workplace. This may lead to them extending the time at which they wish to start a family. Children are also expensive to raise and today’s youth are not reaching the same financial milestones at the same time as their parents did.
We also have to factor in affordability as another contributor as more women are medically insured making C-sections more accessible than ever.
Across the world, however, researchers continue to ponder why C-sections have gained such popularity. Some say it is the perceived rise in health problems associated with natural birth and even a fear of natural childbirth, while others say expectant mothers increasingly want more control over their delivery dates.
Of course, I would never downplay the importance of a C-section. It is a procedure that has saved millions of mothers’ and babies’ lives when natural birth put them in danger. At the end of the day, however, it is undoubtedly a woman’s right to choose how she gives birth. DM
Comments
Scroll down to load comments...