



See Part 1 here:
This week, Minister in the Presidency and anti-apartheid and UDF activist, Jackson Mthembu, passed away from Covid-19 complications. One of the brave doctors trying to save his life, Dr Kgopotso Rudolph Mononyane, died shortly thereafter in a tragic helicopter accident, along with his Netcare colleagues: surgeon Dr Curnick Siyabonga, specialist nurse Mpho Xaba, advanced life support paramedic Sinjin Joshua Farrance, and pilot Mark Stroxreiter. Our condolences go out to all of their families, friends and colleagues, and everyone else who lost loved ones this week. They were at the very frontline of workers who are bravely, and at great cost, holding this country up in this pandemic. I do not know how we comfort them or address the worrying mental health impact of this pandemic on health workers and other frontline workers, especially as the daily case numbers and fatalities come in.
As of 22 January 2021, hardly any family, school, place of worship, or community has not been directly or indirectly affected by Covid-19 – with more and more people experiencing either severe symptoms, including prolonged difficulty with breathing, or worse, death, with no realistic and safe means for proper burial rites, something so important to many people in our country. These are not ordinary times.
And this is why, in a pandemic, facts, truth and transparency matter. Critically, so does political power and the systemic barriers to access to life-saving interventions.
A moral catastrophe
This week, the Director General of the World Health Organisation (WHO), Dr Tedros Adhanom Ghebreyesus, at the 148th Executive Board session of the WHO, in his opening speech, warned of a “catastrophic moral failure”. He shared that by mid-January 2021, only 25 vaccine shots had been administered in low-income countries (LICs) (outside of clinical trials), while richer and middle-income countries (49 of them) had already commenced, albeit uneven, vaccination programmes from December 2020, with approximately 39 million dosages administered so far.
The Second Report on Progress Prepared by the Independent Panel for Pandemic Preparedness and Response released this week, also warns about the grave impact of inequity in current global vaccine distribution, acquisition plans and programmes, showing an entire continent (Africa) with no mass vaccination programmes as at mid-January 2021, severely delaying the possibility of global population immunity considerably, possibly even to 2023.
The lack of planning by global institutions, governments and big business, including the pharmaceutical corporations responsible for bringing vaccines to market, to address equity, early on, based on health and epidemiological needs, rather than nationalism, is now having a dire impact on the world’s ability to achieve rapid, widespread, global population immunity – meaning, literally, no one is safe even while vaccination programmes are being rolled out. This is best illustrated below:
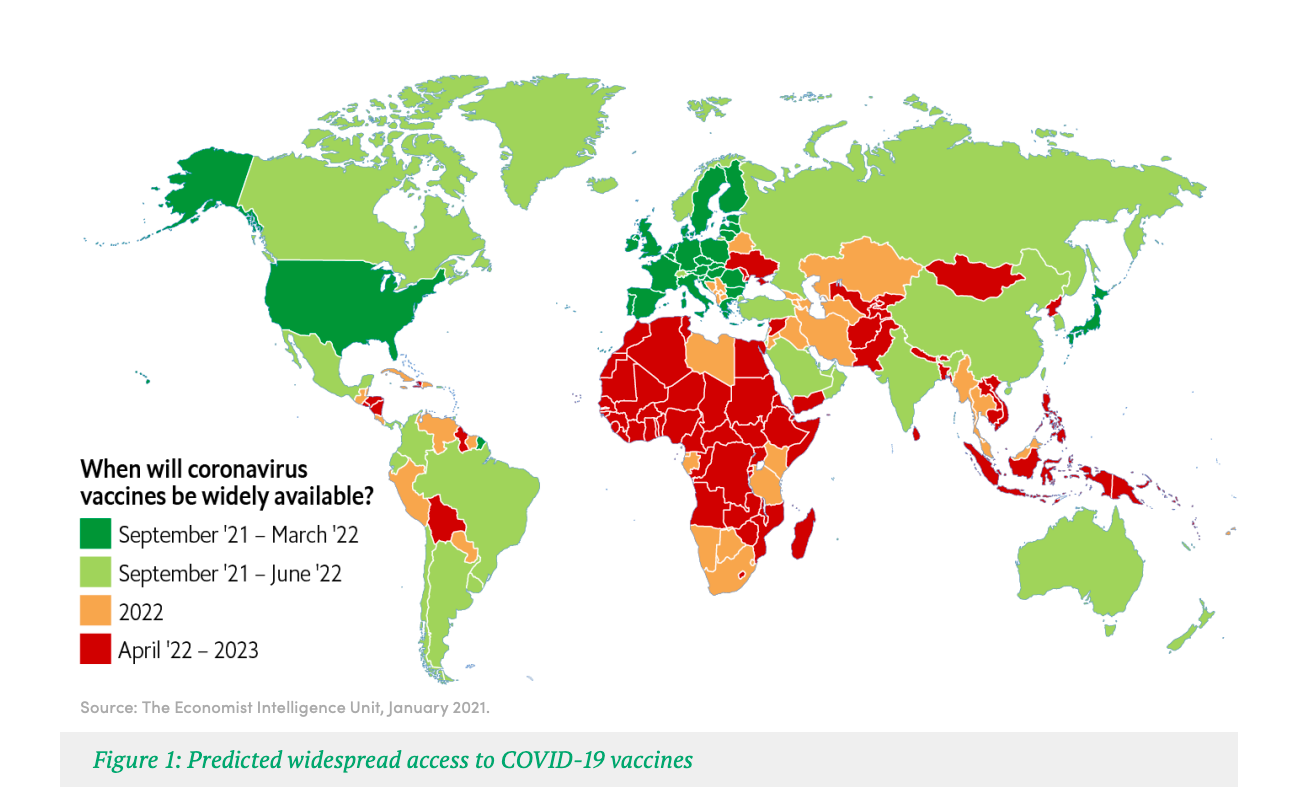
Source: Second Report on Progress Prepared by the Independent Panel for Pandemic Preparedness and Response
For this reason, now, more than ever, we need greater transparency, but also accurate information. This week we had truly little of it. Which brings me to the Moderna saga.
The great Moderna fib…
The so-called “Moderna vaccine” is not just the Moderna vaccine, but rather a vaccine that was co-invented by the US government’s National Institute of Allergy and Infectious Diseases (NIAID) and Moderna, with more than a billion dollars of US taxpayer money (see: U.S. funded Moderna vaccine, with notable private donation (usatoday.com)
The NIAID/Moderna vaccine involves the use of technology invented by the US government, protected by US government patents, which Moderna likely infringes on. This could represent billions of US dollars of infringement liability for Moderna, if the US government decided to enforce them, as it has previously done against pharmaceutical giant Gilead, whose price gouging on HIV PrEP led the US government to sue it in 2019.
In the driving seat here is the US government. It can actually compel Moderna to share the technology, require it to serve LICs as well as submit its data dossier to medicine regulators in South Africa. Activists in the US have argued that the Biden administration should compel it now.
Moderna in fact is a small company, with no head office in South Africa. It has never brought a product to market here – or before Covid-19, anywhere – according to experts we have consulted. Let alone ‘40 million’ of anything by mid-2021.
Along with other global activists, we have been monitoring Moderna closely these last few months – because the NIAID/Moderna vaccine is a suitable vaccine for most places, because it has a valuable, mRNA technology platform (simple explainer: it allows you to rapidly design and scale-up production of a vaccine far faster than other technologies) which has some cold storage needs, but much less than the Pfizer vaccine.
It is a feasible vaccine for rapid manufacturing scale-up in and for the global South, developed with the support of US government funding. It will now seek to sell its vaccine to the US and EU, and other so-called “rich” nations. But no one else.
It will charge approximately $18.00 per dose for the EU and $16.50 for the US. Yet, scientists and engineers at Imperial College London have estimated that the cost to make a jab of the NIAID/Moderna vaccine is actually around $2 per dose.
Other companies, such as AstraZeneca for example, are charging the EU €1.78; J&J $8.50 and Pfizer/BioNTech, €12.00. Meanwhile, this week, it emerged that Serum II / CIPLA (sub-licensees of AstraZeneca) will be charging South Africa at least 2.5 times more than the EU price for the AstraZeneca vaccine, despite AstraZeneca promising a worldwide ‘no or low-profit price’ for the ‘duration’ of the pandemic.
We only know these price differentials because the EU price list was mistakenly, but fortuitously for access advocates, posted on social media by a Belgian government official, since removed (see below).

Hope is for the rich
The NIAID/Moderna technology is the hope we all needed in this pandemic.
But globally, Moderna only plans to make enough doses, in the “best-case scenario”, for 500 million people – less than 7% of the world’s population. See Moderna Provides COVID-19 Vaccine Supply Update | Business Wire. Moderna is trying to shatter that hope for everyone living in the global South – not just South Africa.
Thrice now, our own government has stated to the nation, that Moderna has unilaterally decided, even though it had considerable US government funding support, that it does not “wish” to supply South Africa and that it does not “wish” to submit its clinical data/dossier to SA’s medicine regulator, SAHPRA, for approval. For its own commercial reasons.
So, this week, when much was made about the (false) hope created by a Moderna official – (since Moderna has not publicly said that the description of that call with a columnist who writes for Business Day and the Sunday Times is incorrect, we must assume it is a fair record of the call) – we were distressed, because false hope is distressing.
On this call, the official purportedly said that Moderna could “supply 40 mill dosages to SA by mid-2021” if “asked” to do so. This is strange because, based on information available to us at present, it is not possible, making it untrue. It is sad and regrettable to play with people’s hopes and lives like this.
And quite apart from my own organisation and others’ outrage with the national department of health and government’s awfully slow and non-transparent vaccine planning and negotiations, coupled with, as yet inadequate planning – even with business and medical scheme representation, and the National Treasury, among others – this added a new dimension. It created the impression that Moderna actually cares about us – and other LICs and MICs – and it created an impression that our lack of access to this particular vaccine is only about our inability to make the right and urgent calls.
Maybe because of this saga, Moderna will voluntarily (or if compelled by US government action) reverse its harmful, conditional, time-bound position. But, a bit of fact-checking and pre-research would have revealed that Moderna has said that while it will not enforce some of its IP rights during the pandemic (see above its own possible patent infringements) it will not submit a clinical dossier to SAHPRA; and it will not enter LIC markets including South Africa; and that despite this business or market preference decision, it will also not share the vaccine know-how, with anyone else, who is willing to do so on its behalf, for countries such as ours, that are not considered a priority “during the pandemic”, even if our country is being devastated by this pandemic. Further, it is, however, willing to do so (share IP) for the “post-pandemic” period only – which is so open ended that it is impossible to determine when that period even commences.
At present, Moderna has not even joined COVAX.
COVAX and C-TAP
This week COVAX made much of a minuscule amount of vaccines now pledged by Pfizer for LICs (2% of its total 2021 supplies, for LICs). Yet COVAX is not, bizarrely, ringing the alarm bells – to warn the world that the current vaccine supply shortages are a global emergency. Instead, it gives ridiculous reassurances about an inadequate plan to support only about 27% of LIC’s populations, to be vaccinated by the end of 2021, that most experts agree is too little, too late, and will result in mass death and the emergence of vaccine-resistant variants that will threaten global health and vaccine equity. Equally alarming is that much of COVAX’s portfolio relies on vaccines that have demonstrated efficacy that is lower than what was seen with the NIAID\Moderna or Pfizer\BioNTech vaccines.
Like every other diagnostic, pharmaceutical and vaccine manufacturer, Moderna has also to date not joined the WHO’s ‘C-TAP’ mechanism (the WHO Covid-19 Technology Access Pool) – which is also regrettably premised on voluntary technology sharing and pooling. Knowledge Ecology International (KEI) has written more about this here.
Critically, vaccine production especially is going to be more difficult to scale up, without the explicit cooperation from companies such as Pfizer, Moderna, Johnson & Johnson, AstraZeneca – all of whom have not yet joined C-TAP.
And, while we may have limited recourse against Moderna in South Africa, we are not totally powerless in the way that the DDG of Health makes South Africa out to be. Though it may be a difficult and tough task, state action should be attempted. And because the US government-funded and supported the research work of its government scientists to develop this particular vaccine, the new Biden administration could step in. Or we need a Presidency-to-Presidency intervention effort.
Public Citizen has also reported on this aspect. It has also been reported in the US that “Moderna has not been living up to contractual obligations (with BARDA) to disclose the percentage of (US) taxpayer dollars … for funding its coronavirus vaccine project” and that US federal money makes up “100% funding of the program”. Further, it is reported that Moderna “received almost $1 billion in taxpayer grants to get its vaccine through clinical trials” all while setting the highest price of all coronavirus vaccine candidates. See more details here.
So, the questions that the media and our legislature should be seeking to answer are:
- Why is Moderna deliberately creating a false impression and not accurately showing all of its research funding sources?
- Was it instead making a joke, in a pandemic, on that call?
- Is perhaps our own government misrepresenting what Moderna said in its bi-lateral discussions?
- Is the columnist misrepresenting what transpired on that call?
- And why is the company and our very own GCIS not providing timely and accurate information or responses on this matter to the public?
Accurate Information matters in a pandemic
We have previously battled quackery and disinformation during the worst years of the HIV/AIDS crisis. Many people got sick and died as a result. The most egregious and unforgivable forms were when someone made a medicine access promise that never materialised, or deliberately made false statements, or lied about a false cure, or made up an “ARV deal”, and the worst: charged an excessive price so that poor people could not benefit from scientific advancement; or when a drug company that had the technology and know-how to save a life or millions of lives, refused, for no good reason, to speedily share that know-how through voluntary licensing agreements that never once took away their right to make a reasonable profit. Instead, without state measures, often, we used more public money to pay higher prices for medicines, needlessly, wasting valuable public resources. We still do.
For years, while more and more people got sick and died, we begged the world, including our government, richer nations, and all the captains of industry, to get drug companies (whose profit margins exceed that of the oil and gas industries) to make their know-how available, especially those companies that benefitted from tax breaks, public investment and research support. They mostly refused. They litigated against governments, including ours, they defended the indefensible and encouraged other governments to place us on “trade watch lists” while people were getting sick and dying. Right now, in Geneva, they are opposing the TRIPS “temporary and special Covid-19 waiver” request. And so, in this crisis too, instead of being able to rely on the WHO to take us out of this pandemic, we have to, worryingly, rely on a global trade body – the World Trade Organisation (WTO) to do so. A body made up of nation states with multiple vested business interests, where medicines are still treated as a luxury, as a commodity, like a perfume, and not as a public good.
Yes, the stakes are high when you take on pharmaceutical power. The real consequence of being placed on trade watch lists, or not receiving research funding, ordinary funding, or clinical trial work, for many, are severe. Very few can speak out against their practices.
This is why Covid-19, and its mismanagement by global actors, must lead to an alteration of this state of affairs and the status quo. It is not working as is.
Why transparency and written assurances matter
Any global medicine access advocate will tell you, never trust press statements, phone calls or the fluffy words of any pharmaceutical company official, government official, or regulatory authority, even if they are from the WHO and UN, alone. Always insist on confirmation and legally enforceable guarantees, and specific details, in writing. The very same advocates will tell you, in a pandemic, where sickness and death are the norm, never rely on “fluff”. With Covid-19, NGOs acting in the public interest have repeatedly asked the pharmaceutical industry and its CEOs to commit to greater licensing and price transparency – see for example the recent CSO letter to CEOs here.
The demands are simple: full transparency including on pricing and “pledges”; share vaccine know-how and not enforce IP claims in a pandemic; share doses with developing countries; help others to make more doses of vaccines.
Transparent pricing and global benchmarking are also key so that we can compare what we pay here in South Africa versus Egypt versus Canada v the EU v the USA for the same vaccine. It is a simple request, yet even COVAX is refusing to make its price list available for a drip-feed supply of vaccines to poor countries in 2021 and 2022.
Pricing
Fortunately, the mistakenly tweeted price list for the EU, shows us quite clearly, that the EU got some really great deals as a bloc, partly because it invested in some research (notably BioNTech, the research partner for the Pfizer vaccine) and because it used its economic and political bloc power to pre-reserve supplies in a pandemic, for itself, before the trials were completed, data reviewed, or any vaccine approved for use (it hedged). Some of these EU agreements are now being investigated, and potentially may be publicly shared, if activists there succeed with their transparency filings. In turn, the USA has realised it paid more, much more, for certain vaccines. It is unclear what state action it will take now under its new administration. But no one has seen all of these contracts.
This week we learnt that South Africa – and other countries that are compelled to buy the AstraZeneca/Oxford University vaccine exclusively from Serum II/CIPLA – due to market segmentation by AstraZeneca and its exclusive sub-licensing deal with it, and in turn, Oxford University (and various research units there) – must pay several times more than the EU is paying for the same vaccine. Yet, again, no one has seen the non-redacted versions of the contract/s.
The AU, through AVATT, it appears, has negotiated lower prices, seemingly on the same level as the EU. But no one has seen those contracts either.
COVAX is not disclosing its prices either, so no one knows how the tiered COVAX pricing list compares to that of the EU and US, or even the AU and other bilateral agreements. And tiered pricing in a pandemic is a significant contributor of unequal access and inequity in the race to vaccinate the entire world, speedily. And when a low-income country pays more than a high-income country for the same medicine or vaccine, or a private health facility user or medical scheme member (medically insured) pays more for the same medicine than a public health facility user, for no good reason, we call that “pandemic price gouging”. Yet, with all of these arrangements, the public must pay for the vaccine and its rollout in multiple ways.
And the way in which all of these vaccine acquisition global mechanisms have been set up (like little shops, in a very big private shopping centre), alongside nation state bilaterals, with multiple venture and private capital actors, with little to zero transparency, means that while the public funds several vaccination research, acquisition and rollout programmes, the public cannot get answers to questions about the conditions, timing, distribution, quantities, price arrangements, licensing terms – nor hold companies, and even COVAX, C-TAP and the AU to account as yet, because domestic regulation and oversight are being surreptitiously undermined and eliminated through NDAs and one-sided confidentiality undertakings. DM
The author would like to acknowledge the contribution of Matthew Kavanagh (Georgetown O’Neill Institute, USA) and James Krellenstein (PrEP4All, USA) in finalising this article.