


 A new ruling by the North Gauteng high court says specially trained pharmacists can now prescribe anti-HIV drugs, including antiretrovirals (ARVs) or a daily HIV prevention pill, without patients having to see a doctor. (Photo: Chemist 4 U / Flickr / Spotlight)
A new ruling by the North Gauteng high court says specially trained pharmacists can now prescribe anti-HIV drugs, including antiretrovirals (ARVs) or a daily HIV prevention pill, without patients having to see a doctor. (Photo: Chemist 4 U / Flickr / Spotlight) South Africa came one step closer to getting everyone diagnosed with HIV on treatment that will prevent them from transmitting the virus after last week’s ruling by the North Gauteng high court that gave the go-ahead for pharmacists to prescribe anti-HIV drugs. The court judgment makes it easier for HIV-positive people to get antiretroviral drugs (ARVs) or for those who are HIV-negative to use a daily HIV prevention pill because they won’t first have to see a doctor.
When someone with HIV takes their daily ARVs correctly, it becomes virtually impossible for them to infect others through sex, because the medicine suppresses the virus in their bodies to levels too low to transmit it.
South Africa currently struggles to get enough people who know they have contracted the virus on ARVs.
The latest figures from Statistics South Africa show that 7.94-million people in the country are estimated to have HIV. From this, and using the health department’s data on the proportion of people diagnosed and on treatment, 8.45-million people know they’re infected and 6.11-million of them are on ARVs — in other words, 2.34-million HIV-positive (both diagnosed and undiagnosed) people are not on treatment.
The court decision follows after a doctors’ group called the Independent Practitioners Association Foundation took the South African Pharmacy Council (SAPC) to court in 2022 for starting the Pharmacist-Initiated Management of Antiretroviral Treatment (Pimart) programme. Through this programme, pharmacists would be able to, once having completed a training course and obtaining a special permit for dispensing schedule 4 drugs, advise clients on taking ARVs and follow their treatment.
ARVs are classified as schedule 4 medicines according to South African law, and so should conventionally only be prescribed by a doctor, says the Medicines and Related Substances Act.
The World Health Organization (WHO) says that widening the circle when it comes to managing patients’ primary healthcare — such as for treating or preventing HIV infections — is a good idea.
Why?
Because the easier it is for people to get ARVs, the closer we’ll be to ending the epidemic by 2030.
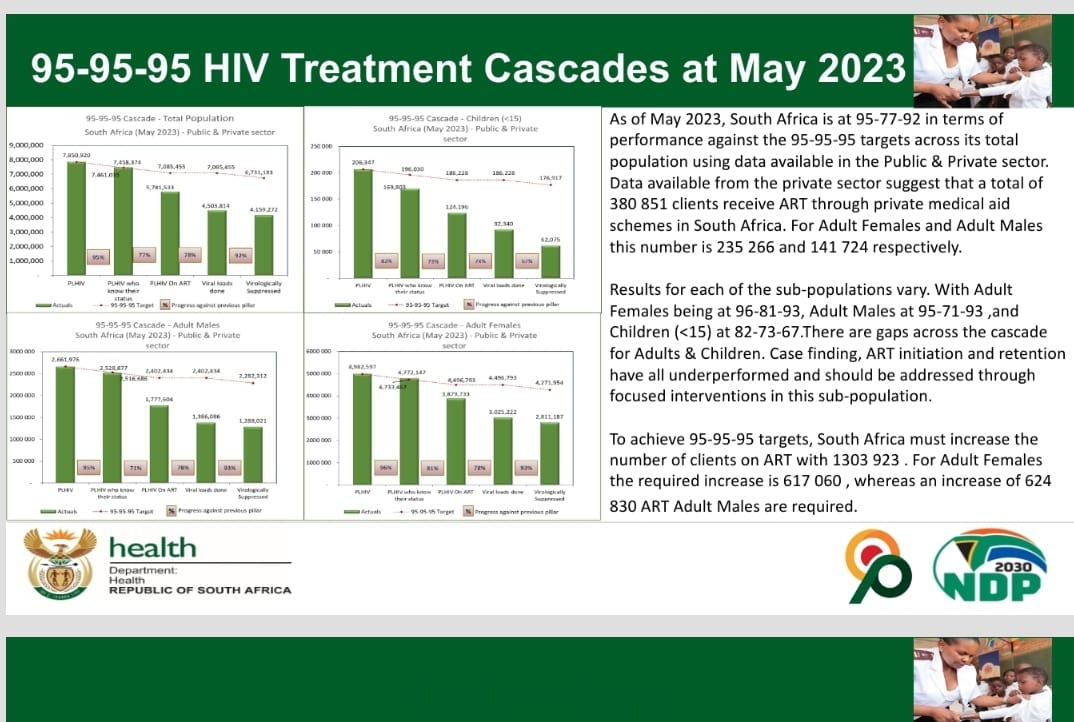
In order to do this, the Joint United Nations Programme on HIV and Aids wants all member countries to reach something known as the 95-95-95 goals by 2025. That means governments, including South Africa, would need to have, by 2025, 95% of people with HIV diagnosed, get 95% of diagnosed people on ARVs and, in turn, get 95% of those on treatment to have viral levels so low that they can’t infect someone else (called viral suppression).
But, as figures from the health department show, we’re far behind on the second 95: getting people who know they have HIV to take up treatment.
Knowing our numbers
By May, 95% of people with HIV in South Africa knew they were infected. But only 77% of them were on ARVs. And of those, only 92% were virally suppressed.
{kind=link}
“We’re not satisfied with where we’re at,” says Thato Chidarikire, the health department’s acting chief director for HIV, when asked about the country’s progress on our 95-95-95 goals.
New guidelines from the WHO, released in July, could help to change the picture, though.
Generally, when there are fewer than 20 copies of the virus in a millilitre of blood, someone is said to have an undetectable viral load (that is, the amount of virus in the body) and the virus is virtually untransmittable. This idea is called U=U: undetectable equals untransmittable.
Now, the WHO says that if someone has a viral load anywhere below 1,000 copies per millilitre — which will still be picked up by a test — the infection is controlled enough that there’s an “almost zero or negligible risk” of passing HIV on to a sexual partner.
/file/dailymaverick/wp-content/uploads/2023/08/MC-HIV-Bhekisisa.jpg "To help people get — and stay — on treatment, we have to make access to medication easier. (Photo: Hoseya Jubase)")
Treatment gap
Why does South Africa struggle to get diagnosed people on treatment — and help them to stick to it?
Francois Venter, executive director of the Ezintsha research centre at the University of the Witwatersrand, explains: “People may be in denial [after being diagnosed], feel stigmatised or be scared. Or the health services may be unfriendly or inaccessible.”
To keep viral levels suppressed, someone with HIV has to stick to their treatment — meaning taking ARVs for the rest of their life. But, says Venter, this is hard — despite side effects of the medication as a reason for people to stop taking their pills being “vanishingly rare” now.
“New drugs have far fewer side effects, to the point that almost all patients tolerate their drug combinations extremely well. We also see far less [drug] resistance — there’s more forgiveness for the occasional lapse in adherence. [Treatment] really is so much easier than before,” he says.
So, why the difficulty in keeping people on their pills then?
Says Venter: “It’s all social — just the chaos of everyday life. Changing jobs, provinces, moving house, stresses. You name it. There are so many reasons for interrupting therapy, and the system doesn’t make it easy to move clinics or to come back after you’ve stopped your treatment. The healthcare workers routinely yell at you. It’s a huge disincentive to come back.”
How to get to the finish line
Chidarikire agrees. To help people get — and stay — on treatment, we have to make access to medication easier. South Africa already follows a differentiated service delivery model, she says, as recommended by the WHO. This means that instead of having a one-size-trying-to-fit-all approach to HIV treatment, the way people get tested and treated for HIV is adapted to fit their circumstances.
“We may have reached the first 95, but the second and third [ones] still need a lot of effort, both on the demand and supply side,” she says.
Enters Pimart. Under this programme, someone can go to a qualifying pharmacy (that is, one that has a section 22A(15) permit) to get HIV prevention drugs, have an HIV test or pick up their ARVs — without having to see a doctor first for a prescription. If this is close to where they live or work, and if the process is fast and efficient, it will be easier for people to stay on treatment or protect themselves from getting infected in the first place.
In the case of treatment, pharmacists will only be allowed to issue first-line ARVs (the first type of regimen — in the form of a three-in-one daily pill — that a newly diagnosed person is put on).
But getting your HIV treatment from a private pharmacy won’t be free. Pharmacists will be able to charge the single exit price for the medicine plus a professional fee, as set by the SAPC. The cost of treatment in the private sector therefore could be a barrier to people who use government facilities, says Andy Gray, senior lecturer in pharmacology at the University of KwaZulu-Natal.
“PrEP [pre-exposure prophylaxis in the form of a daily HIV prevention pill] may be a more affordable option and may be more widely used by key populations [groups who have a bigger chance of getting HIV than the general population, such as sex workers and men who have sex with men] and who are being missed by the public sector now.”
Yet, says Gray, someone who doesn’t (want to) use the public health system can now choose to go to a private pharmacy instead — even if they have to pay for the pills themselves (or claim it from their medical aid).
Despite having to pay for the medicine, Natalie Schellack, a professor in pharmacology at the University of Pretoria, said at an SAPC press briefing last week that the hidden expenses of getting treatment, such as travelling to a government facility and waiting in line, add considerable cost to treatment — which could make getting your pills at a private pharmacy attractive.
Indeed, studies show that having HIV services like testing and medicine collection at a private pharmacy ups the demand for these. Moreover, clients who choose to have a trained pharmacist follow the progress of their ARV treatment get to viral suppression just as well as patients who are treated by a doctor.
Gray adds that Pimart also offers an opportunity for the government programme to expand access to ARVs by potentially supplying free state stock to these pharmacies, in the same way as getting childhood vaccines or contraceptives via a private facility, even when the pharmacy can charge a service fee.
The health department has not yet announced whether they will have such partnerships with private pharmacies. Bhekisisa has asked the health department for a response and we will update the story once they have responded.
In July, the WHO also said that using a spot sample of dry blood for a viral load test at a clinic can help to check how well people are doing on their medication, especially in rural areas where it might be difficult to get liquid samples to a lab. For this, someone’s finger is pricked and a drop of blood is dabbed onto a special paper card, which is then analysed.
Will these plans get us to our 95-95-95 goals in the next year and a half?
“It’s complex,” says Venter.
“We’ve done the easy stuff. The last 20–30% will take far more effort to work out. I suspect making both testing and getting on treatment easier will go some way in getting us there, but not all the way.” DM
This story was produced by the Bhekisisa Centre for Health Journalism. Sign up for the newsletter.
![]()
Comments
Scroll down to load comments...