


 (Photo: bizcommunity.com / Wikipedia)
(Photo: bizcommunity.com / Wikipedia) The National Budget tabled on 24 February 2021 by Finance Minister Tito Mboweni represented a mixed bag for healthcare funding over the next three years. While some commitments, including strengthening the National Health Insurance office and money being allocated to Covid-19 vaccine procurement are certainly needed, the outlook for expenditure on healthcare as a whole is not as hopeful. In real terms, the budget for healthcare will shrink substantially over the next three years and many crucial programmes, including those addressing HIV and tuberculosis.
Despite the significant and necessary investment in Covid-19 vaccines, overall, planned spending on public health is reduced by a massive R50.3-billion over the next three years. The allocation to Covid-19 vaccines has come at the expense of other vital health services, rather than a small increase in taxes, which Treasury had said it was considering in January.
Cutbacks in healthcare budgets result from the National Treasury’s dual obsessions with debt stabilisation and giving kickbacks to the rich through tax breaks, seemingly at all costs. While debt sustainability — though hard to define — is essential, funding socio-economic rights is an equally important constitutional imperative. Treasury must urgently reconsider its austerity model for public budgeting and instead use the budget to protect and promote hard-won human rights through budgets that are sufficient, equitable, efficient and effective.
In the face of cuts, and in order to maintain and improve the quality of and access to healthcare services, Treasury has demanded “increase[d] efficiency” from health departments. Provinces are encouraged to be “economical” in their spending on centralised procurement of goods, reduce variations on unit costs in the HIV programme and improve overtime management costs. While there may be room for savings in these areas, provinces already lack the capacity to manage health effectively and the latest round of budget cuts jeopardise the constitutionally mandated improvement of service delivery in healthcare.
Healthcare spending per user is shrinking
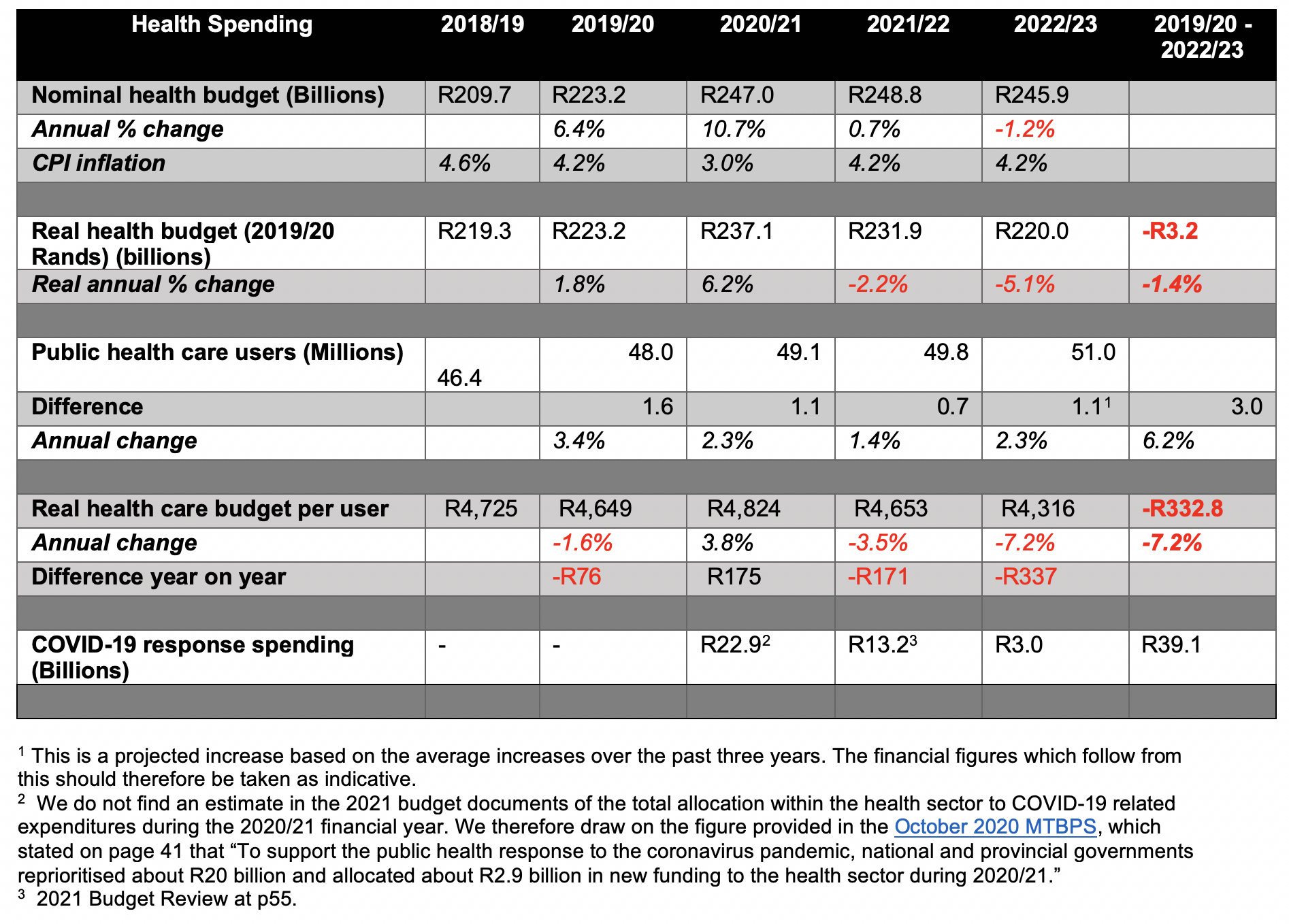
Table 1 shows that when CPI inflation and the projected increase in the number of public healthcare users are accounted for, the real value of spending going towards public healthcare services diminished in 2019/20 and will continue to decrease over the next two years.
While the health budget grew in nominal and real terms overall in 2020/21, this was almost entirely due to the R23-billion of estimated spending on the Covid-19 pandemic. In 2021/22, R13.2-billion is allocated for the Covid-19 vaccine rollout and the management of further waves of infections, but the overall budget for health care is reduced by -2.2% in real terms. Given the additional 700,000 users of the public health care system, this results in a reduction in spending per user of -3.5%, or R171 less per user.
Further reductions in health care funding in 2022/23 reduce the budget by a very large portion: -5.1% in real terms, or -7.2% per health care user, by our projections. Overall, between 2019/20 and 2022/23, the government’s austerity programme will have reduced the value of the health budget by approximately R3.2-billion. In other words, by 2023, the government will spend about R332.80 less per health user than it did in 2019.
These decreases in health funding not only risk a deterioration of existing access to health care services but effectively delay the implementation of National Health Insurance by a further three years at least.
Reduction in HIV conditional grant
Planned spending on the HIV, TB, Malaria and community outreach grant to provinces has been reduced by a total of R5.8-billion over the Medium Term Expenditure Framework (MTEF) (-4.5% in 2021/22, -5.9 in 2022/23 and -10.4% in 2023/24). The real value of these reductions is considerable for the next three years. As the biggest conditional grant in health, this grant has become a catch-all for funding of multiple programmes as provincial budgets have been squeezed in recent years. The grant now provides funding for HIV/AIDS and TB, malaria, community outreach, human papillomavirus vaccines, and now also mental health, oncology and Covid-19.
Despite adding yet another component to this grant, Treasury admits that it will receive “no additional funding” over the medium term. While an injection of money to address Covid-19 is obviously necessary, the fact that this has resulted in the sharp reduction of funds allocated to other essential areas of health care is extremely concerning.
In the medium-term strategic framework of 2019-2024, government committed to combat HIV/AIDS by ensuring that 95% of people living with HIV know their status and 95% of those diagnosed are started on antiretroviral treatment by 2024. In its attempt to achieve this goal, government had proposed in 2019 that R74.9-billion be allocated to reach over seven million people by the end of 2022.
What we see in this budget is severe backtracking on these objectives, threatening not only the rights of people living with HIV but also the realisation of South Africa’s UNAIDS 90-90-90 targets. The HIV and AIDS component of this grant has only been allocated R69.3-billion over the MTEF period (R5.6-billion less in nominal terms than what had been proposed for the grant in 2019), with the aim to provide antiretroviral treatment and related HIV-prevention services to only 6.7 million people by 2023/24. The diminishing funds allocated to fight HIV, and government’s apparent lack of ambition to reach all the people who need treatment and support for HIV, is disturbing.
The mental health component of this conditional grant is allocated R317-million over the medium term, while the oncology component has been allocated R335-million. We welcome these allocations and look forward to hearing from the Minister of Health how mental health and oncology services — two areas of infamous weakness — will be improved with this new allocation.
Both the national and the provincial departments of health have been allocated funding under the Covid-19 component of the conditional grant. The national department will use the funds to purchase vaccines, and the provinces will administer them. However, the severe cuts to the health sector wage bill raise questions about how the administration of vaccines and other vital health care services will occur with fewer staff members in health facilities. Health worker vacancy rates estimated at 40,000 in 2018 across the country continue to put people at risk. The National Treasury’s obsession with reducing public sector wage costs will entrench these widespread staff shortages for years to come.
We cannot accept a vaccine versus health system trade-off. Government must both expedite the procurement of vaccines and ensure that provinces have the staff and other capabilities to roll them out rapidly and to maintain and improve the quality of healthcare services.
Primary health care services and National Health Insurance
The long-awaited National Health Insurance (NHI) will rely on a strong primary healthcare system that can efficiently cater to everyone. This will create opportunities for large savings in health expenditure by reducing the need for oversubscribed and more expensive tertiary care. The biggest cut within the health budget this year, however, is to the primary health care programme, which sees a decrease of -6.6% over the next three years. While there are allocations for establishing the NHI Fund (R121.3-million) and for some NHI interventions (including private sector contracting), the already struggling primary healthcare system will be further weakened by this cut, thereby delaying the implementation of NHI for years to come.
Reductions to healthcare facility revitalisation funding
For the health facility revitalisation grant, tasked with construction, upgrading and maintenance of health infrastructure, the Division of Revenue Bill states: “The fiscal consolidation reductions to this grant are equivalent to 2.7% of the grant’s baseline in 2021/22, 2.6% in 2022/23 and 2.2% in 2023/24.” This does not consider inflation or increased pressure on healthcare facilities due to projected increases in numbers of healthcare users over the medium term, as described above. R140-million has been taken from this grant and the National Health Insurance indirect grant to fund shortfalls for community service doctors and medical interns. While junior doctors are crucial to the functioning of our health system and their compensation is definitely a priority, what we see here is an illustration of the austerity mindset in Treasury where money is being taken away from areas that need it to fund other necessary goals.
Maintenance of and revitalisation of unsafe or overburdened healthcare facilities is crucial to the long-term functioning of our health system. These cuts, therefore, jeopardise the realisation of National Health Insurance and the sustainability of the South African health system.
National tertiary services grant
For the national tertiary services grant, which aims to strengthen specialised services in the 29 hospitals of the nine provinces, R13.7-billion over the MTEF has been allocated and R204-million reprioritised from this grant to develop and expand tertiary services in the Eastern Cape, Limpopo, Mpumalanga and the North West for 2021/22. We welcome this allocation considering the unequal distribution of funds to provinces, where rural settings are under-resourced. This will go a long way to ensuring people have access to tertiary services in their own provinces. While such an allocation is essential during the Covid-19 pandemic, we note that the next two years have been left unallocated. The need to invest in tertiary services in under-serviced provinces has been a standing call by health users and activists long before the current crisis. This needs continued investment and special prioritisation for the next two years and beyond. However, it remains pertinent that the shift to primary health care should entail a gradual reallocation of resources from the tertiary sector to the primary sector. Such reallocation could be indirect by increasing spending in the primary sector quicker than increasing it for the tertiary sector.
While we recognise the need for debt sustainability, the deprioritisation of socio-economic rights like the right to access healthcare in the national budget jeopardise South Africa’s prospects for long-run economic growth or a health system that is sustainable, equitable and effective. DM/MC
Daniel McLaren is a budget analyst at SECTION27, Mbali Baduza is a legal research in the health rights programme at SECTION27, Sasha Stevenson is the head of the health rights programme at SECTION27 and Julia Chaskalson is a communications officer at SECTION27.
*NOTE: Spotlight is published by SECTION27 and the TAC, but is editorially independent, an independence that the editors guard jealously. This is an opinion article and the views expressed in it are not endorsed by Spotlight.
Information pertaining to Covid-19, vaccines, how to control the spread of the virus and potential treatments is ever-changing. Under the South African Disaster Management Act Regulation 11(5)(c) it is prohibited to publish information through any medium with the intention to deceive people on government measures to address Covid-19. We are therefore disabling the comment section on this article in order to protect both the commenting member and ourselves from potential liability. Should you have additional information that you think we should know, please email letters@dailymaverick.co.za.