


 A taxi marshall helps with the registrations of passengers before conducting their Covid tests at a testing facility set up in the Park Station taxi rank in Soweto. Passengers are required to produce a certificate declaring they are not Covid positive before boarding a taxi. (Photo: Shiraaz Mohamed)
A taxi marshall helps with the registrations of passengers before conducting their Covid tests at a testing facility set up in the Park Station taxi rank in Soweto. Passengers are required to produce a certificate declaring they are not Covid positive before boarding a taxi. (Photo: Shiraaz Mohamed) Peter van Heusden
On 14 December 2020 the Western Cape health department restricted access to Covid-19 testing for the second time in the year, excluding most of those under 45 and all of those without symptoms from access to public-sector testing (see here).
The reason is that the public-sector testing system was fast becoming overwhelmed, not just in the Western Cape but also in other provinces now facing a surge in cases.
For example, in the Eastern Cape public pathology system, the National Health Laboratory Service (NHLS), it took on average two days to get a Covid-19 test result at the end October. By the end of November it was taking four days. Of the 28 labs in the NHLS system, only one had a turnaround time of more than two days at the end of October. By the end of November 13 of the labs were taking more than two days to get a test result back.
The new rules from the Western Cape health department were expected: Earlier in 2020 it took more than 10 days to get some Covid-19 test results back. However, as with the rest of South Africa’s health system (where, for the time being, the National Institute for Communicable Diseases (NICD) guidelines are still in effect in the public sector), the divide between public and private sector leads to test inequity - about half of the tests done in South Africa are done in private-sector labs where testing is largely available to anyone who will pay.
This means those resources are effectively reserved for 15% of our population.
When, earlier in 2020, Dis-Chem took money from the Solidarity Fund to offer testing to those who could not pay, the system it set up was quickly shut down when cases surged and testing capacity was overwhelmed.
Public-private divide
The public/private divide affects the way tests can be used and, crucially, the information available for making Covid-19-related decisions. Infected people are often contagious before they have any symptoms. This is particularly concerning with regards to those working with “confined groups” such as old-age home and care-home residents and prisoners, since waiting for someone to become visibly sick before being tested could expose others around them.
Young people also typically have less severe disease. I wonder if the outbreaks at the Tin Roof party in Cape Town and Ballito Rage would have been detected at all if the young people involved came from families without access to private-sector testing.
At the start of the pandemic the NHLS promised it would soon be able to do 30,000 tests a day. That goal was never reached, in part because of an international scramble to secure testing supplies and predictable logjams favouring richer countries. (For analysis of previous shortages see Kavanagh et al in the Lancet and Nkengasong in Nature.) Polymerase chain reaction-based (PCR) Covid-19 testing requires a substantial investment in equipment that in turn relies on testing supplies that are often proprietary and specific to the machines they are bought for.
Before a test is done the sample needs processing. When this is done by hand it is labour intensive but automation of this process requires yet more expensive equipment and consumables. This all makes PCR testing slow and expensive - the exact price varies depending on where it is done, but it is close to R1,000 per test.
Problematically, neither the public nor private sector has been open about the details of their operations, which makes it difficult to assess the overall capacity of the system and where resources might be better allocated.
Finally, Covid-19 is by far not the only disease laboratories have to cope with; amid the pandemic they need to keep up with TB and HIV testing and other workloads as well.
My personal experience of this system is often as my social group’s “go-to” person for advice on Covid-19 and testing:
A friend’s daughter got an exposure notification from the Covid-19 Alert App: Could she safely see her mother? A colleague discovered that he had been exposed during a work-related event. Where could he go? A child and a family friend both had symptoms, of varying severity, which might or might not be Covid-19. What next?
As a result, testing in the public sector raises questions of criteria to be matched and delays to be concerned about. The private sector is a dizzying array of options and procedures.
I fear that many avoid all of this complexity by just avoiding testing altogether.
Glimmer of hope
Luckily there is a glimmer of hope: On 17 December the Africa Centres for Disease Control and Prevention (CDC) released guidelines for the use of antigen-based rapid diagnostic tests (RDTs) (see news report here). These tests, which look rather like a pregnancy test, go from swab to result in 30 minutes, without the need for specialist laboratory staff.
They work by being coated in antibodies that bind to the protein shell of the SARS-CoV-2 virus. The antibody binding causes a notable colour change.
RDTs are a lot cheaper than PCR tests, at less than R150 per test.
Two of these RDTs have been licensed in South Africa - the SD Biosensor Standard Q and the Abbott Panbio Covid-19 Ag - and the Partnership to Accelerate Covid-19 Testing, an AU/CDC initiative, is securing 11 million tests for distribution throughout the continent.
These RDTs are not perfect: They are a little bit less sensitive than the PCR test, which means there are some people infected with the virus that would be picked up by a PCR test but not by the RDT. Although, in the early period of infection, when the virus is growing fast inside the body and infectiousness is climbing, results from RDTs agree well with PCR tests. In fact, the Abbott test licensed in South Africa has been shown to agree with PCR in this period more than 90% of the time.
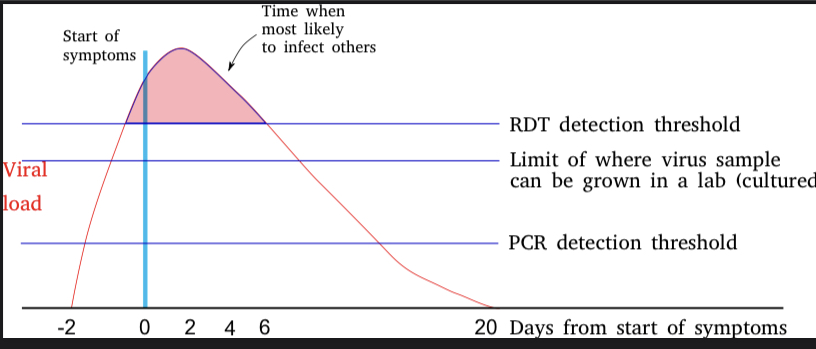 Diagram adapted from WHO training materials
Diagram adapted from WHO training materials
In May, some South African TB experts called on the country to learn from our experience with drug resistant tuberculosis, where South Africa was a leader in rapid adoption of new diagnostic tests and rapid research on how best to use these. But it seems that message has not been heard, since in October the South African Medical Association’s National Pathology Group opined that “further field evaluation data and more experience with these tests need to be gained before these assays can be safely and confidently used”, while the Department of Health only proposed the use of RDTs in airline passenger screening (for which, ironically, WHO does not recommend their use).
Now, as case numbers once again disable the PCR testing mainstay of the country there is an urgent need to consider alternatives.
As the CDC puts it: “As the continent witnesses new spikes in Covid-19 cases and deaths, the commission calls on member states to prioritise rollout of rapid antigen testing as part of an urgent effort to increase national Covid-19 testing capacity and better manage the pandemic, towards achieving test positivity rates of less than 5%.” (Test positivity in South Africa exceeds 20%)
There will be challenges adopting this new technology.
Reporting results from distributed testing in many locations will require new systems for capturing results. While RDTs don’t require specialised lab personnel these are still not “at home” tests are required a trained medical technologist to perform the test. Regularly repeated nasopharyngeal swabs are not pleasant and less-invasive sample-collection methods should be investigated (Internationally there is active research on swabbing the front of the nose or using sputum samples).
In addition, having only two licensed suppliers of RDTs is close to “vendor lock-in”. As with so much other Covid-19-related technology, the rollout of antigen RDTs is wrapped up in patents and other intellectual property barriers that turns each device into a “single-supplier” item. South Africa (along with India and other countries) is challenging WTO TRIPS rules that allow monopolisation of the Covid-19 response, but for now licensing of additional tests should be encouraged to ensure that a number of competitive suppliers of tests are available and to drop the price of Covid-19 even further.
Finally, testing needs to be demystified and democratised.
Like with HIV testing, Covid-19 testing faces issues of education and stigma. This stigma has already affected mask-wearing habits and the adoption of the Covid-19 Alert App, and countrywide conversations and education are needed about what we can all do to live health-promoting lives during a pandemic. Those who do test positive need support for themselves and their families.
Hopefully, soon the message to mask up, sanitise and keep physical distancing can be supplemented by another: Get tested and embrace your status! DM/MC
Peter van Heusden is a bioinformatician working at the South African National Bioinformatics Institute, specialising in the analysis of infectious pathogens. He is also a member of the C19 People’s Coalition Health Working Group. He is writing in his individual capacity.